This is my largest article, roughly 15k words and most in-depth to date, so I decided to split it into two parts. Part 1 covers COVID19 and everything I could gather on it. Part 2 covers the conspiracy theories behind COVID19. This is a long read so I created a table of contents to make it easier to navigate. This article links to the most up-to-date information I could find at the time of publication. As time progresses some of the information found in this two-part article could be determined untrue based on additional research and studies. Always remember to think for yourself and learn to process information using the Trivium Method of Critical Thinking: Grammar, Logic, and then Rhetoric in order. This is my rhetoric.
Table of Contents
Part 1 (this article)
- Introduction
- What is a virus? How does COVID19 differ to other viruses that we deal with on a daily basis?
- What is the origin of COVID19?
- How is COVID19 transmitted?
- What symptoms does COVID19 produce? What type of immunity do you get? How does COVID19 affect the human body?
- How is COVID19 being tested and determined? What do the official numbers tells us? Can those number be trusted? What risk are we at? How far widespread is COVID19?
- Do masks help protect you and others from COVID19? How can COVID19 be treated?
Part 2
- Why are critical thinking skills lacking in society? What is a conspiracy theory?
- What does 5G have to do with COVID19?
- Who is Bill Gates and what does he have to do with COVID19?
- What does the future hold?
Introduction
Life changed as we know it when we entered 2020. Gone are the times where even the semblance of freedom was fallaciously assumed available for everyone. Schools across the world have been shuttered, people are being arrested or murdered for stepping outside of their homes, and freedoms and liberties have been suspended indefinitely to combat a virus, called COVID19 (2019-nCov or SARS-CoV-2), which was classified by the World Health Organization (WHO) as causing a world-wide pandemic. This event has become the new 9/11, but for the entire world. Governments around the world have said a shutdown of “non-essential” businesses are required to flatten the curve of infection rate, and that this shutdown is needed until a vaccine has been developed and given to the population of Earth; forcing herd immunity. Flattening the curve is used to describe keeping the healthcare system operational without overloading it due to COVID19 cases, even though hospitals around the US are furloughing healthcare workers because the hospitals are empty. There are only so many beds available at any given time for all people who require medical help. Government has shutdown many aspects of the healthcare industry due to it deeming the medical exams and procedures as “non-essential”, which is very subjective. Many “non-essential” medical exams and procedures have been forcefully canceled by governments with the understanding it is to help keep medical supplies available to those who need it during this time of high infection rate and “unrest”. This government shutdown in the US has caused close to 40 million Americans to be unemployed. A virus didn’t cause that. Millions in India are facing starvation because their government shut down the economy. They aren’t the only ones. Everything is being done in the name of protecting and serving the citizens of each government… or is it? Before we go into the current and future state of society let’s go over what viruses there are and how COVID19 affects people.
What is a virus? How does COVID19 differ to other viruses that we deal with on a daily basis?
Organisms are entities that have the properties for life; “an organism refers to a living thing that has an organized structure, can react to stimuli, reproduce, grow, adapt, and maintain homeostasis.” For centuries scientists have struggled to define what a virus is. Is it alive or not alive? Afterall, living and non-living entities are made up of atoms and molecules. Viruses are poison, a potentially deadly infectious agent that typically consists of a nucleic acid molecule (DNA or RNA), usually in a protein coat (not always), that is usually too small to be seen by light microscopy (not always), is only able to multiply within a living cell (really it is the living cells that replicate viruses), cannot generate its own energy, cannot translate the DNA sequences of its genes into proteins, and can direct its own reproduction by taking control of the cell it invades (Roossinck, Marilyn J. Virus: An Illustrated Guide to 101 Incredible Microbes. Ivy Press, 2016). Viruses can range in many different sizes and shapes and can cause many different types of symptoms. Viruses are not alive or considered a living entity. Viruses only become prominent when our natural living cleansing processes (phagocytosis, bacterial, fungal, and parasitical) are weakened or sterilized within our immune system. When we are surrounded by toxic pollution, poor air/water/food quality, nutritional imbalances, and overly used medical treatments (antibiotics/medications) these living processes are weakened or sterilized. These living processes are critical for our survival.
COVID19 is a class of Coronavirus, a novel betacoronavirus from the subgenus Sarbecovirus, which coronaviruses are considered to be a type of common cold that is associated with upper respiratory tract infections. Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) are two types of coronaviruses that were identified in the past two decades which has caused outbreaks at various times. Coronaviruses account for 15% to 30% of the common colds tested for with only six strains being able to affect humans, at least until now. The other type of common cold that makes up the rest of the cases are Rhinoviruses, which can be broken down into more than 100 various strains that can affect humans by manipulating genes which brings an excessive immune response leading to cold symptoms. Influenza (flu viruses), type A, B, and C viruses, are similar to common cold viruses but are usually more severe with the symptoms that become present. I bring up Influenza since many use Influenza statistics to make infection and mortality comparisons to COVID19.
What is the origin of COVID19?
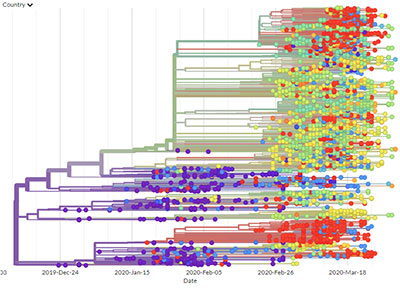
COVID19 was first discovered in the capital of the Hubei province, Wuhan, China in December of 2019. Through investigation China was able to narrow down patient zero, the first individual to contract COVID19, to a pool of 266 potential patient zeros dating back to November 17th 2019. The Chinese government has made the suggestion that COVID19 was brought by US military athletes during the war games that they participated in Wuhan, China that was held October 18-27, 2019. Reports suggested COVID19 hit Europe in October after the World Military Games. Even though a lot of evidence suggests COVID19 as being man-made, the mainstream assumption being made by some scientists, and what is officially being pushed by governments, is that COVID19 might have jumped to humans from a wild bat. This has caused many to blame people for eating bats, even though it is a food source like every other animal. However, this is only an assumption and not a fact since they can’t even pinpoint who was patient zero. The Nextstrain project, a real-time tracking of pathogen evolutions which started in 2017, has identified 8 different strains that have mutated from the original one discovered in China based on samples from different countries.

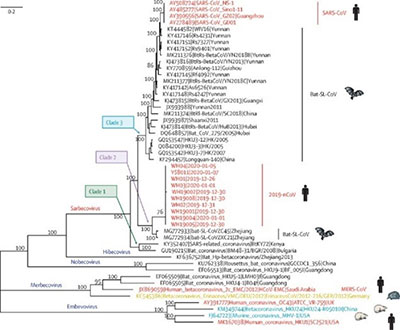
COVID19 has been determined to be an 88% match with two bat-derived SARS viruses, bat-SL-CoVZC45 and bat-SL-CoVZXC21, a 79% match with the human virus SARS-CoV, and a 50% match to MERS-CoV. Through additional investigation scientists from the Institute of Virology in Wuhan, China, where this pandemic is assumed to have started, concluded that COVID19 actually came from a horseshoe bat species, Rhinolophus affinis, located in the caves of Yunnan, China. They were able to determine this from a sample of feces that they collected in 2013 and had “forgotten” about until January 2020 when they retested the sample discovering that the sample contained COVID19. This sample was housed at the Level 4 biological lab that is stationed in Wuhan, China, which is located less than 20 miles from the open market initially claimed to be the site of the first case. There seems to be a lot of coincidences with this non-man-made virus, but I will go into those details further down in this article. The similarity between COVID19, the two bat-derived viruses, and the sample from Yunnan caves is why the assumption is being made that this pandemic of COVID19 came from someone eating a bat. Because that is the only possibility, right? Again, the idea that someone ate a bat and got infected is still only an assumption being pushed, it is not a fact. More reports continue to come out making reference that this is actually a man-made virus.
To add to the confusion of the origin of COVID19 a team of scientists in India, from the Indian Institute of Technology, concluded that there are four different “insertions in the spike glycoprotein (S) which are unique to the 2019-nCoV and are not present in other coronaviruses” and that “each of the four inserts aligned with short segments of the Human immunodeficiency Virus-1 (HIV-1) proteins. The amino acid positions of the inserts in 2019-nCoV and the corresponding residues in HIV-1 gp120 and HIV-1 Gag. The first 3 inserts (insert 1,2 and 3) aligned to short segments of amino acid residues in HIV-1 gp120. The insert 4 aligned to HIV-1 Gag. The insert 1 (6 amino acid residues) and insert 2 (6 amino acid residues) in the spike glycoprotein of 2019-nCoV are 100% identical to the residues mapped to HIV-1 gp120. The insert 3 (12 amino acid residues) in 2019-nCoV maps to HIV-1 gp120 with gaps. The insert 4 (8 amino acid residues) maps to HIV-1 Gag with gaps.”
What this means is that their conclusion for COVID19 is that this new virus is probably man-made since evolution and mutation of these inserts together could not have happened in nature. Granted, this study has since been withdrawn after its release and without being peer-reviewed. Another study at NIH bashes the India study by making the claim that conspiracy theories about COVID19 being man-made have been fully debunked in the media. This assumption that COVID19 made the jump from bat to human could easily be a fallacy, but I will cover this further down and go into the different conspiracies circulating. One point that I want to make is that the peer-review process has been broken since it started. One NIH study states “we have little evidence on the effectiveness of peer review, but we have considerable evidence on its defects”. Fraud is rampant within the scientific community with a lot of political money being handed out due to these fraudulent studies and reports in all scientific fields and studies. On the other side, studies that show the truth can be forced to be withdrawn to hide the corruption that has been established. This must be taken into account when reading any study. Scientists from China warned that COVID19 attacks the human immune system and causes damages similar to HIV which could give credence to what the scientists from India discovered.
How is COVID19 transmitted?
COVID19 is mainly transmitted through respiratory droplets and physical contact. It is also found in the fecal matter of those infected. COVID19 can be caught through a person’s mouth, nose, or eyes. Dr. Christian Drosten, a virologist of Berlin's Charité, explained in an interview that COVID19 is extremely sensitive to drying out, which makes catching COVID19 outside of inhaling respiratory droplets rare. Through an analysis of cases in China airborne transmission was not reported unless a person is within close contact with an infectious patient, usually one meter or less. In Germany, Dr. Hendrik Streeck, said there is “no significant risk of catching” COVID19 through shopping activities like going to the grocery store, restaurants, or barbers and hairstylists. Dr. Streeck further explained that to catch COVID19 on surfaces the virus would need to be coughed into the hand of an infectious person who immediately touches a surface then directly after another person touches that same surface and then touches their face allowing for infection. In the New England Journal of Medicine a study found that COVID19 was viable up to three hours in air, up to four hours on copper, up to 24 hours on cardboard, and up to 72 hours on plastic and stainless steel before becoming completely inactive. The CDC has even reported that COVID19 does not spread easily on surfaces. A small case study of the infectivity of asymptomatic COVID19 carriers concluded that out of the 455 contacts who were exposed to asymptomatic COVID19 carriers no one showed signs of COVID19 infection indicating that COVID19 asymptomatic COVID19 carriers had a weak infectivity rate.
What symptoms does COVID19 produce? What type of immunity do you get? How does COVID19 affect the human body?
So, what happens when you catch COVID19? COVID19 symptoms can “include fever, dry cough, fatigue, loss of appetite, loss of smell, and body ache” and with severe symptoms like “high fever, severe cough, and shortness of breath, which often indicates pneumonia”. It is also being reported that COVID19 patients are developing heart problems, which is leading to cardiac arrest and death even without respiratory distress. There are also reports that patients are seeing liver damage from COVID19. Those who recover can have lasting damage to their lungs, heart, and liver. In Italy autopsies have shown that patients are dying from Thrombosis and Pulmonary Embolisms, blood clots, which is also being seen in the US. These blood clots can still kill a patient days to months after COVID19 symptoms have vanished.
Doctors and scientists are reporting that when a patient is reinfected by COVID19 (this shows no lifetime immunity) that the mortality rate is a lot higher than with the first infection. These reinfection reports could be false positives due to the test not being able to distinguish between the genetic material of an active or inactive virus fragments. On top of these symptoms, and the possibility of reinfection, people can be asymptomatic (being infectious but showing no signs of symptoms) up to 28 days before the onset of symptoms. It has been seen in some studies that COVID19 is most infectious while the patient is still asymptomatic. Some researchers are claiming that 25% to 50% of those infected with COVID19 stay asymptomatic and never develop symptoms. Dr. Andrew Kaufman, an undergraduate of MIT who once worked for the CDC collecting information for AIDS cases, has come out on his YouTube channel going through the various case studies since COVID19 was discovered and showed how all of these studies are flawed and that none of them established the connection between the COVID19 virus and the symptoms. All of these studies make assumptions which further establish a potential rumor as fact. Dr. Andrew Kaufman pushes that real research needs to be conducted so we can get to the truth instead of making plans that are affecting millions of people based on flawed science.
Everyone’s immune system is different based on their environment, diet, and general health. Immunity is important in fighting against diseases and viruses. We can have either short term (passive immunity) or lifetime immunity (active immunity). Short term immunity is when someone, like an infant, gets antibodies from someone else, like a mother. These antibodies help fight back infection and symptoms but the body does not produce more and needs to be supplied over and over. Over time the antibodies become less effective at providing protection as the years pass. Vaccines only provide short term immunity which is why many have started to come with boosters for adults later in life. Lifetime immunity is when our bodies fight off the infections and produce the antibodies themselves. Once this occurs the body knows how to produce these antibodies for life. On April 24th 2020, the WHO made a statement that “there is currently no evidence that people who have recovered from COVID19 and have antibodies are protected from a second infection. Why would the WHO make this statement when there are doctors and scientists who are coming out saying there should be lasting immunity when catching COVID19 in nature and producing antibodies naturally? Professor Dolores J. Cahill, PhD, an immunologist and molecular biologist of Ireland was interviewed by Del Bigtree where she said that once you are infected with COVID19 and start producing the antibodies you are immune to COVID19. Why is there such a big disconnect within the scientific community?
Now that we know what symptoms COVID19 can produce; how is COVID19 potentially causing these symptoms? COVID19 attacks the heme, what gives myoglobin and hemoglobin the ability to bind oxygen when an iron atom is present, by removing the iron atom from the cell allowing it to roam free in the blood stream which forms porphyrin. Too much of porphyrin can lead to porphyria, which can also occur when someone is over exposed to an excess of iron or they have HIV. Also, COVID19 has been shown to attack and damage T lymphocytes, a type of white blood cell that helps the immune system fight infection and cancers which is also being compared to HIV. More evidence to that indicate this virus was possibly man-made. COVID19 causes hemoglobin levels to drop reducing the oxygen in the blood, thereby increasing carbon dioxide levels, carried to organs through the blood. When this happens the lungs get poisoned and inflamed due to the inability of the lungs to exchange oxygen and carbon dioxide resulting in pulmonary nodules forming in the lungs that have a ground-glass opacity to them. For those constantly wearing masks then their carbon dioxide levels are significantly elevated. Low oxygen levels can result in hypoxemia which can lead to additional organ damage or death. COVID19 can also lead to things like cytokine release syndrome (a cytokine storm), which is “an overproduction of immune cells and their activating compounds—cytokines—which, in something like a flu infection, is often associated with a surge of activated immune cells into the lungs. The resulting lung inflammation and fluid buildup can lead to respiratory distress and can be contaminated by a secondary bacterial pneumonia. This increases the risk of mortality in patients.” Having underlying health conditions can make this whole situation even worse. A difficult challenge when trying to determine cause of death is that COVID19 seems to cause other issues that can cause death so if someone dies from a heart attack and they have COVID19 was it due to an underlying condition and triggered by COVID19 or due to some other cause.
How is COVID19 being tested and determined? What do the official numbers tells us? Can those number be trusted? What risk are we at? How far widespread is COVID19?
Testing is a major factor in determining how dangerous a virus truly is. Without proper testing official numbers can be off by a wide margin. Testing is so new that it is hard for some of the tests to determine the difference between various coronaviruses and COVID19, so if you have a common cold coronavirus there is a potential for you to test positive. COVID19 false-negative rates have been found to be as high as 30% meaning you could test negative but still be infectious and show symptoms. The current testing kits have a high potential, nearly half or more, false-positive rate for individuals who are “asymptomatic” while being in close contact with COVID19 patients. What this means is that if you are near someone who has COVID19 you could test positive without ever actually catching COVID19. With testing kits people need to worry about contaminated products. Testing kits that were heading to the UK were found to be contaminated with COVID19 which causes the virus to spread.
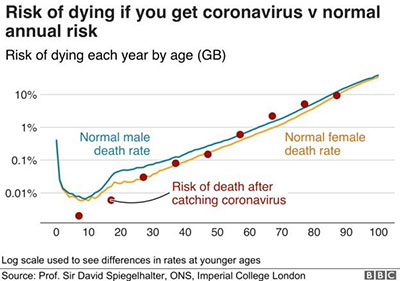
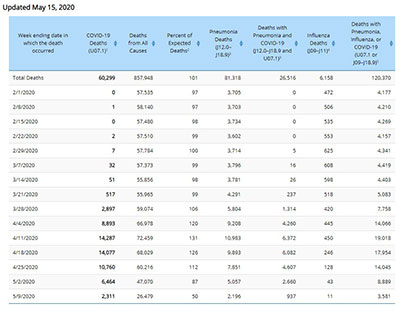
As of May 16th 2020, the US officially announced that it had 1,507,773 cases, 90,133 deaths, and 339,232 recovered based on reported numbers (Worldometers.info). This would indicate that the 90,113 deaths out of the 429,345 closed cases the mortality rate is 21% (21,000 per 100,000). You can’t use active cases to determine mortality rate since those cases still need to either become recovered or proceed to death. 21% is scary, right? Are you this scared? Because a 21% mortality rate is pretty high. However, the CDC has quietly updated their stats and downgraded the COVID19 deaths from the 90 thousands to 60,206 as of May 15, 2020. This new figure would mean the mortality rate is around 14% (14,000 per 100,000). This is still very high for a mortality rate, but if that is true are you really seeing that anywhere around you? Professor Sir David Spiegelhalter, a statistician from Cambridge University, plotted the risk of mortality by age for COVID19. This chart indicates that COVID19 is nowhere near the risk nor mortality rate that officials claim it is.
By looking at the current official numbers COVID19 seems a little worse than pneumonia and flu. The problem though is that Influenza/pneumonia mortality rate is .0096% to .02561% depending on the state you are in. However, official numbers can be false and manipulative. Is that the case here? On May 22nd 2020, the CDC released new guidance claiming that its best estimate is that 0.4% (1.3% for 65 and older and 0.05% for 49 and under) of those who show symptoms with COVID19 will die. This would indicate that the actual mortality rate is much lower than that bringing it to the influenza/pneumonia range or lower. Recently, California San Diego County Supervisor Jim Desmond officially said that the County’s 194 COVID19 deaths had only “six pure, solely coronavirus deaths” due to the other 190 have other underlying health conditions. I have seen dozens of similar individual reports online over social media during April and May 2020 that explained a loved one was expected to die and when it finally happened the loved one was listed as a COVID19 death baffling the family. Washington State Department of Health openly stated and confirmed that gunshot victims were being counted as COVID19 deaths. Can you still trust them after you hear that Japan ended their coronavirus emergency with only 850 deaths and they didn’t shut down/destroy their economy to survive? So again, can official numbers really be trusted? No, they can’t.
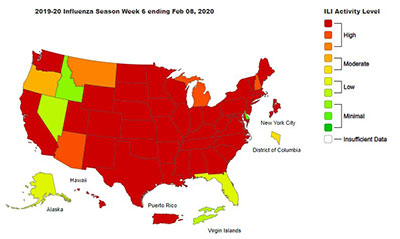
Reports from Chicago show that 30% to 50% of those tested for COVID19 antibodies already have them in their system, which means they were infected and recovered without being listed as official COVID19. In Boston reports are now showing 10% of the residents have had COVID19. These uncounted cases were either seen at a hospital and diagnosed as something else (Influenza and pneumonia) or the individual never went to a hospital. This indicates that the mortality rate is much lower than the officials claim and could be more around the Influenza and pneumonia mortality rate than what the official numbers suggest. As antibody testing becomes more prevalent it is showing that COVID19 is way more widespread, and was spreading in communities a lot sooner than governments suggested. Antidotal personal accounts further show that COVID19 was actually circling communities in the US as far back as December, maybe sooner. I have talked with some who were really sick in December, weren’t sick since, and later went back for testing which showed a positive test result for COVID19 antibodies. However, the CDC recently updated their website acknowledging that the COVID19 antibody tests are only 50% accurate. Is this true or only a lie to distract from the proof COVID19 was more widespread than officials claimed? 33 US States reported a significant increase for flu-like symptoms and pneumonia during January and February. It is possible many doctors made the assumption that the illness was the flu and flu induced pneumonia, however, some of this increase could have also been caused by COVID19.
Were you in panic and fear for your life back in December, January, or February? No? If you are now, why? Knowing about a risk doesn’t necessarily change that risk to you. You’ve only reduced the risk of the unknown. COVID19 was already affecting communities around the US without causing mass panic or requiring everyone to give up their rights and livelihood. So why is it necessary to restrict the Natural and Constitutional rights of everyone for months or longer? That is not how rights work nor does any Constitutional authority grant the government the ability to suspend rights during a pandemic. The government does not have a right to force you out of business nor force you to stay at home by executive order. You are being lied to and manipulated.
On top of all of this, how cases are classified are extremely important. Dr. Deborah Brix, with the CDC, openly stated that all deaths that involve someone who also tested positive for COVID19 will be classified as a COVID19 death. This is pure sophistry and a manipulation of data that makes it seem like COVID19 is worse than it really is. The CDC also has reported that it believes that the death toll is likely higher than what is being official reported. Why would they do this though? Let’s look at New York, which has the highest cases and deaths out of the entire US. In January of 2020 New York Governor Andrew Cuomo was facing a $6.1 billion dollar budget hole which he was looking to cut $2.5 billion from Medicaid. Now, for each COVID19 pneumonia case Federal Medicare, under the Coronavirus Aid, Relief and Economic Security Act, pays $13,000 per case (normally pneumonia cases are $5,000) and up to $39,000 for each case that is put on a ventilator. New York lists all presumed COVID19 cases as official, which is allowed by the CDC, resulting in larger payouts. There are ethical and moral conflicts of interest happening with no accountability. Staggeringly, a study in New York involving 5,700 COVID19 patient records found that 88% of those patients who were put on ventilators die. As of May 16th 2020, New York has 358,099 “official” cases with 28,134 deaths. COVID19 could be a massive financial windfall for the cash strapped New York healthcare system. Ventilators force air into the lungs, but the lack of air in the lungs isn’t want is causing the low oxygen levels; the inability of the body and lungs to convert oxygen into the cells and bloodstream is what is causing the low oxygen levels. Ventilators need to be calibrated correctly for each patient; too much oxygen and the lungs get damaged while too little and the brain and kidneys become damaged, but too much air pressure and the lungs become damaged while too little and the patient doesn’t get enough oxygen. This calibration would be a moving target too as the COVID19 infection becomes better or worse. Doctors and other medical professions around the world are beginning to recognize the issues with ventilators and starting to move away from them as a treatment except for the rare extreme cases. This is because ventilators can damage the lungs further and should only be used when a patient is already unconscious and not able to breath on their own. Putting a conscious COVID19 patient, who can still breath on their own, into an induced coma and placing them on a ventilator which could be what is killing them, not COVID19. It is a potential and massive ethical and moral violation when hospitals and doctors have the ability to push the use of ventilators which can directly affect their wallets. Remember, 250,000 deaths a year are due to medical malpractice. Are your medical professions qualified and have extensive experience using ventilators?
To further explain the disconnect between reality and the official numbers government and mainstream media has pushed let’s look at the field hospitals that were hastily built to handle the influx of COVID19 patients we were told to expect. A Brooklyn field hospital that cost $21 million to construct shut down after seeing zero patients. Army’s Seattle field hospital closed after three days of being open without seeing or treating any COVID19 patients. The University of Kentucky’s $7 million dollar field hospital was closed after never being used. Joint Base Cape Cod in Michigan closed its COVID19 field hospital without seeing a single patient. This has been the scenario for most, if not all, hastily built field hospitals in the US. This shows that the models being used to predict the level of suspected COVID19 patients is vastly overreported. How much money has the government wasted in setting up these field hospitals only to take them down without being touched?
Do masks help protect you and others from COVID19? How can COVID19 be treated?
Now that we understand how COVID19 affects the human body, do mask protect us and others, and how can COVID19 be treated to reduce the potential of damages and mortality? Masks can be important when dealing with sick people but is it really needed for everyday life? Cloth masks cannot stop COVID19 as the virus particles are smaller than what cloth can stop. You are doing nothing to protect yourself when using cloth masks. This goes for anything not an N95 respirator mask. Even surgical masks do not really protect us or others from the virus if it is in the air as most masks are loosely put in place. Even the CDC said it “does not recommend that people who are well wear a facemask to protect themselves from respiratory diseases, including COVID19”. Even the WHO recommended that only those treating sick patients should wear a mask. Mask restrict oxygen from getting to your lungs which reduce the oxygen level in your blood and tissue. Having long exposures to wearing a mask can lead to hypoxia and hypoxemia which can and will make COVID19 worse if caught. Drivers are already starting to pass out while driving with a mask, and children have started to drop dead in China for wearing masks while conducting physical exercise. Even though there are health risks with prolonged use of masks businesses are facing hefty fines of $10,000 or more, or closure, for not following coronavirus rules. These aren’t private businesses making private decisions. This is being forced by government. Dr. Fauci, a leader in Trump’s coronavirus task force with strong ties to Bill Gates, says masks aren’t 100% effective (not even close) and further said masks are symbol as respect for others.
Doctors and scientists around the world are scrambling to find a successful treatment for COVID19 trying many options including fast tracking the creation of a new vaccine. While living and interacting with a clean environment (air, water, food) is important for a healthy immune system there are treatments that you can do to help keep for from reaching that point of needing to put your life and trust into others’ hands. Be wary of misinformation campaigns by pharmaceutical companies and governments that try to manipulate you into thinking natural processes do not work and that your only hope is to see help from them. I will not be covering all of the different types of treatments that could be possible, but will cover the main ones that have been used so far. Do not take my word for anything, research everything yourself.
Vitamin C (Ascorbic Acid)
Vitamin C is an antioxidant that can be found in food and dietary supplements. It is used a lot to help boost immune systems, especially when someone has the cold or flu. It has been used to treat patients for a large range of issues since 1550 BC. It has even been used to treat cancers. When viruses and other diseases affect cells, they strip the vitamin C out of the cell making the cell weaker and more susceptible to destruction. Countless studies have shown the benefit using vitamin C with evidence showing the amount of vitamin C that the body can absorbed increases with the damage caused by an issue, e.g. an adult in a normal condition could absorb 4 to 15 grams over a 24 hour period while that same adult with influenza could absorb 100 to 150 grams over 24 hour period. For COVID19, multiple studies and research have shown the effectiveness of taking a high dose of vitamin C through IV. Honestly, this should be the first step hospitals do for any and all sicknesses and diseases, but they don’t. Why do you think that is?
Vitamin D and Magnesium
Symptomatic COVID19 patients, the sickest, often have extremely low levels of vitamin D in their system. Countries with higher mortality rates tend to also have larger rates of vitamin D deficiencies than other countries with lower COVID19 mortality rates. Having healthy levels of vitamin D may provide a survival advantage when the immune system overreacts in the cytokine storm COVID19 seems to produce. One factor in vitamin D deficiency is a magnesium deficiency. Millions of Americans suffer from magnesium deficiency without even knowing it. Magnesium is crucial in body’s ability to absorb and process vitamin D.
Zinc
Zinc is a chemical element that can be found on the periodic table. Like vitamin C, Zinc is considered a dietary supplement that is needed for a health immune system. It is considered an essential trace element and it must be consumed regularly as the body doesn’t store excess. Zinc has been used to treat colds and flus for several hundred years. Some doctors are having success using Zinc with other things, like vitamin C/D and Hydroxychloroquine, to combat COVID19.
Melatonin
Melatonin is a hormone that is primarily released by the pineal gland and has been used to treat various disorders and issues due to its anti-oxidative properties and ability to modulate immune responses. An Italian study shows a correlation between melatonin production and infection rate of COVID19, and explains why children nine and under are not having any fatalities. At this time, I do not believe there are any reports of children dying from COVID19. Our max melatonin production peaks around age nine and bottoms out around age 60. Melatonin is known to regulate biological functions tied to our sleep-wake cycles. Melatonin has been shown to actively inhibit the NLRP3 inflammasomes that cause the pro-inflammatory cytokine storms that COVID19 can cause.
Hydroxychloroquine
Hydroxychloroquine is a man-made treatment that help prevent various types malaria which is common in Africa, South America, and Southern Asia. Hydroxychloroquine, as a malaria drug, stops the parasite from digesting the hemoglobin within a human host. Hemoglobin being a direct target of COVID19. Hydroxychloroquine has been shown to help COVID19 patients recover faster. A 2005 study of Hydroxychloroquine showed that it was a potent inhibitor, strong antiviral effects, for the SARS coronavirus. Further, recent studies in China and Australia show promise using Hydroxychloroquine to treat COVID19. Turkey has claimed success using hydroxychloroquine to treat COVID19. President Trump even publicly stated that he went through a regiment of hydroxychloroquine to ward off COVID19. A study posted in the New England Journal of Medicine looked at 1446 COVID19 patients and determined that “hydroxychloroquine administration was not associated with either a greatly lowered or an increased risk of the composite end point of intubation or death”. Granted, this study states that patients who were given hydroxychloroquine were more severely ill than those given other treatments. This is a flawed study since the baselines between the control groups were not the same.
Ultraviolet Blood Irradiation
Ultraviolet Blood Irradiation (UBI) is a medical process that exposes a patient’s blood to UV light which helps heighten the immune system. Since bacteria and viruses absorb photonic energy at five times the rate as red and white blood cells helping kill the bacteria and viruses and directing the immune system to those specific infections. The amount of treatment depends on the level of care a patient is in need of. UBI was extensively used in the 1940’s and 1950’s to treat a wide range of diseases, e.g. pneumonia or arthritis.
Ozone Therapy
Ozone, a gas consisting of three oxygen atoms, was discovered in the mid-19th century and has been used in many therapeutic treatments by causing the inactivation of bacteria, viruses, and fungi (known to treat as many as 114 diseases) within the immune system. Ozone therapy treatments have been shown to be safe with minimal side effects. In the late 1980’s, Ozone was used to treat HIV infections. In past studies, Ozone has been shown to destroy and damage 99 percent of enveloped viruses, which COVID19 is an enveloped virus.
Vaccines
The WHO says there is no evidence to suggest that the antibodies in recovered patient’s blood will provide long-term COVID19 immunity. This means that a vaccine will probably not grant lifetime immunity, furthermore any coronavirus vaccine that is developed will probably become an annual cold vaccine that goes along with the flu vaccine. Even measles vaccine doesn’t provide lifetime immunity so why would a new coronavirus vaccine provide one? How much do you know about the vaccine industry? Please read my previous article on vaccines “To Vaccinate or Not to Vaccinate: Informed Consent” which I go into detail about what issues there are with vaccines and what ethical/moral conflicts of interest exist within the vaccine industry. The biggest issue that deserves repeating is that vaccines in the US are liability free medical procedures, meaning that if the product injures or kills you or a loved one (like a child) then you must sue the Federal government to seek restitutions. These restitutions are paid out through taxpayer funding leaving the billion-dollar vaccine industry without worry of loss of profits. This should be a major red flag for everyone. In May 2020, the SAGE Open Medicine journal published a study titled “Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders” which came to the conclusion that it was observed that there was higher risk “within the vaccinated versus unvaccinated group for developmental delays, asthma and ear infections”. The study went on to further state that that “further study is necessary to understand the full spectrum of health effects associated with childhood vaccination”. Is science really settled?
With the next round of vaccine advancements Massachusetts Institute of Technology (MIT) researchers are developing an invisible vaccine tattoo that would house all of the individual’s medical history which can be read by a specially equipped smartphone. This is being developed to go with the new digital ID that is coming soon. With advancements in vaccine, e.g. gene therapy and DNA modification, research ethical barriers need to be in place to protect those who would receive these for-profit products. Sadly, with a pandemic government ignores these ethical barriers to push something to the masses. Are you sure government won’t make the next coronavirus vaccine mandatory?
The new coronavirus vaccine is being fast tracked to production, through Trump’s Operation Warp Speed, will be worth billions for the company first to market without having to worry about being sued if their product injuries and kills people. Trump said that this Operation Warp Speed will be “unlike anything the country has seen since the Manhattan Project”. The Manhattan Project being the secretive project to develop the atomic bomb which led to two nuclear bombs being dropped on Japan by the US resulting in roughly 250,000 innocent people being killed. How much do you trust the government? Have you heard of the Tuskegee Experiment? The government infected unaware black Americans with syphilis between 1932 to 1972 to determine how untreated syphilis affected their bodies. As for the flu vaccine, which many are saying can help prevent COVID19, has been shown to make coronaviruses worse: “Vaccine derived virus interference was significantly associated with coronavirus and human metapneumovirus”. There is a good chance that if you get the flu vaccine then get COVID19 the symptoms would be worse. Remember, the flu vaccine is for influenza and cannot fight again COVID19, not the same family of viruses.
Recently, the government and mainstream media has been pushing the results of Moderna Inc., frontrunner to being first to market in the US, coronavirus vaccine research as a major breakthrough. This report and push by government and mainstream media have caused Moderna’s stock valuation to reach $29 billion. This value is for a company that has no products in the market now. Their initial funding came from Merck, the Bill and Melinda Gates Foundation, and the US Department of Health. The problem with their initial report on their vaccine is that it didn’t provide much data nor did it confirm/release any critical proof that the vaccine they are working on works. One thing that is clearly missing from the report is that a large percent of the 45 patients tested by Moderna had severe adverse reactions. Only 8 out of the 45 patients, who were all extremely healthy, were found to get the neutralizing antibodies to combat COVID19. This means this was only an 18% success rate at combating COVID19. Of course, the FDA approved Moderna to enter Phase 2 testing continuing to fast track this company’s liability free product. On top of this, Oxford conducted their own COVID19 vaccine research which had a zero success rate when all monkeys in the trial contracted COVID19. The US government officially announced that they would buy 300 million doses of this Oxford vaccine if the vaccine proves safe and effective. The reason we don’t see a coronavirus vaccine already in use today is due to the challenges in creating an effective vaccine against coronaviruses. All human trails that have been conducted properly have failed and scraped. In 2012, scientists attempted immunization with a SARS coronavirus vaccine showed that all mice exhibited histopathologic changes in their lungs suggesting all had infection which resulted in hypersensitivity to SARS-CoV further showing how challenging attempting a coronavirus vaccine is. It does seem like the only chance a coronavirus vaccine has to be approved for production release is when safety standards can be waived because of an on-going pandemic.
Merck, the $192 billion-dollar pharmaceutical company who has made billions off of vaccines, has now jumped into the race in developing a coronavirus by partnering with the International AIDS Vaccine Initiative (IAVI). Their current goal is to have a “safe” vaccine for the market by mid-2021 with human trials starting in 2020. This will be the least tested product they offer. Remember, Merck’s Vioxx product was pulled in 2004 after causing roughly 88,000 heart attacks and 38,000 deaths. Merck attacked doctors by creating hit lists who spoke out against their product. This wasn’t a liability free product like vaccines are either. Now this corrupt company has jumped into the race for part of the market share of the new coronavirus vaccine.
Johnson & Johnson (J&J) was awarded $456 million from the Trump Administration to develop a coronavirus vaccine. This money comes at a needed time when they continue to become liable for the damage their products have been causing. In 2013, J&J was fined more than $2.2 billion for the “allegations relating to the prescription drugs Risperdal, Invega and Natrecor, including promotion for uses not approved as safe and effective by the Food and Drug Administration (FDA) and payment of kickbacks to physicians and to the nation’s largest long-term care pharmacy provider. The global resolution is one of the largest health care fraud settlements in U.S. history, including criminal fines and forfeiture totaling $485 million and civil settlements with the federal government and states totaling $1.72 billion.” In 2019, a judge ordered J&J to pay $572 million in fines for its part in fueling the opioid epidemic. Being handed half a billion dollars to produce a liability free product, which could net billions, is a no brainer for a company that probably doesn’t actually care about the people that use its products. Are you going to blindly trust this company’s vaccine product when they face no repercussions for the damages their product causes?
This ends part 1 of this in-depth article. Part 2 covers conspiracy theories. Enjoy!
My name is Jeffrey Hann and I'm an anarchist/voluntarist, Army veteran, business analyst, graphics and website designer, and content creator. I have a passion for truth and being logical, which eventually lead me to anarchism. I strive to live my life through voluntary actions and valuing rights. I own Journalistic Revolution (Facebook) and I can be found on Twitter|Instagram|Minds|Steemit|Keybase
If you enjoy my work please think about donating crypto:
- BTC address - 12TLd1xnRXSQZnVfMG8WRUNNF9k4YoKDsc
- ETH address - 0x589BA5535D507999c1413871390554225ae775F6